As I mentioned in my last post, walking has been the cornerstone of my journey toward a healthier life. But honestly? It’s provided so much more than just physical results.
Walking has become my “me time.” It’s when I catch up on audiobooks and podcasts, or use the hands-free time to call mentors, colleagues, and friends.
Most importantly, my walks serve as a sanctuary for reflection and brainstorming—a true mental gym. Inspiration often hits me in the middle of a beautiful morning or while admiring a neighbor’s landscaping. In those moments, I find I don’t want any distractions at all; I just want to think.
The Numbers: A Seven-Month Deep Dive
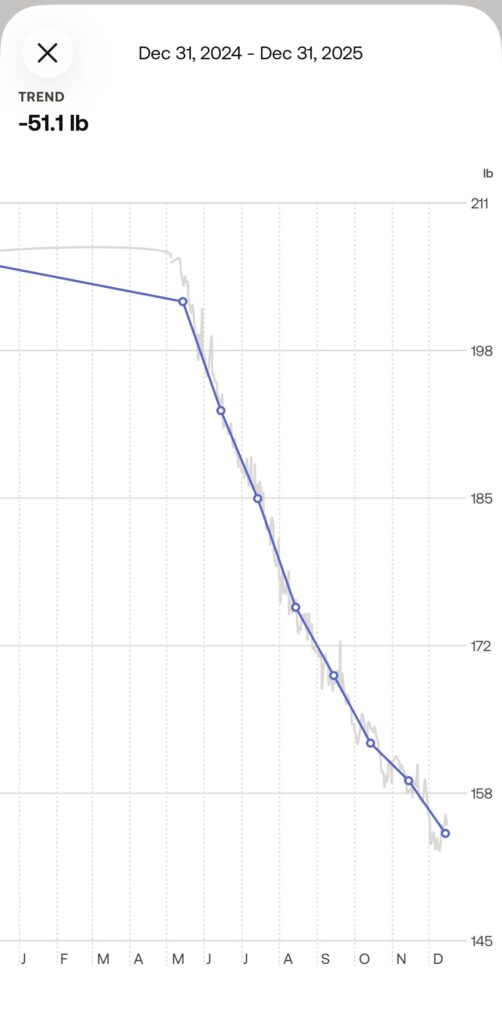
I’m often asked just how much I’ve actually walked since I started this journey in May 2025. When I sat down to look at the data from May through December, even I was surprised:
- Total Distance: 1,422 miles
- Total Time: ~450 hours
- The Big Picture: I spent nearly 19 full days of 2025 just walking.
At an average pace of 19 minutes per mile, it’s a massive investment of time. But looking back? Every single minute was worth it. I love it when people around town or at the office tell me, “I think I saw you out walking the other day!”
Finding the Balance
I’ve reached a point where if the weather is miserable or a meeting runs long and I miss my walk, I feel like something is missing.
However, I’ve had to work on maintaining a healthy relationship with the habit. I’ve come to realize that if I need to skip a day for family or a pressing work deadline, that is okay. Life happens. I do what I need to do, let go of the guilt, and get back to the pavement the next day.
Making it Work (Even When it’s Boring)
I do have a treadmill at home, but I’ll be honest: my brain loses interest after about 3 miles of staring at a wall. To get through indoor sessions, I watch a basketball or football game while I’m walking. It keeps me from obsessing over the fact that I’m walking in place!
My Advice: Just Start
Wherever and however you do it, I highly recommend finding time to move. It’s not about breaking world records; it’s about the fact that motion keeps us alive. It spurs creativity, stabilizes your mood, and (when the sun is actually out) gives you a much-needed Vitamin D boost.
From a fitness perspective, remember: all movement requires energy. Every step gets you further along your journey.
Start small. Walk a half-mile. Spend five minutes of your lunch break circling the building. You’ll notice the benefits almost immediately—and I promise, it will eventually become the part of the day you look forward to most.